Anal Fistula
Surgery is usually necessary to treat an anal fistula as very few heal by themselves.
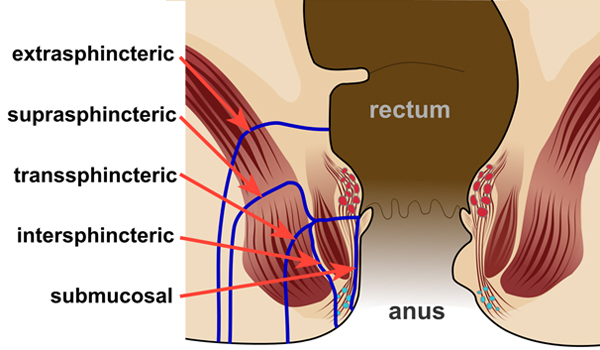
The best option for you will depend on the position of your fistula and whether it's a single channel or branches off in different directions.
Sometimes you may need to have an initial examination of the area under general anaesthetic (where you're asleep) to help determine the best treatment.
Your surgeon will talk to you about the options available and which one they feel is the most suitable for you. Surgery for an anal fistula is usually carried out under general anaesthetic. In many cases, it's not necessary to stay in hospital overnight afterwards.
The aim of surgery is to heal the fistula while avoiding damage to the sphincter muscles, the ring of muscles that open and close the anus, which could potentially result in loss of bowel control bowel incontinence). The main options are outlined below.
Fistulotomy
The most common type of surgery for anal fistulas is a fistulotomy. This involves cutting along the whole length of the fistula to open it up so it heals as a flat scar.
A fistulotomy is the most effective treatment for many anal fistulas, although it's usually only suitable for fistulas that don't pass through much of the sphincter muscles, as the risk of incontinence is lowest in these cases.
If your surgeon has to cut a small portion of anal sphincter muscle during the procedure, they will make every attempt to reduce the risk of incontinence.
In cases where the risk of incontinence is considered too high, one of the procedures below may be recommended instead.
Seton techniques
If your fistula passes through a significant portion of anal sphincter muscle, your surgeon may initially recommend inserting a seton.
A seton is a piece of surgical thread that is left in the fistula for several weeks to keep it open. This allows it to drain and helps it heal, while avoiding the need to cut the sphincter muscles.
Loose setons allow fistulas to drain, but don't cure them. To cure a fistula, tighter setons may be used to cut through the fistula slowly. This may require several procedures that your surgeon can discuss with you. Alternatively, they may suggest carrying out several fistulotomy procedures, carefully opening up a small section of the fistula each time, or one of the treatments described below.
Advancement flap procedure
An advancement flap procedure may be considered if your fistula passes through the anal sphincter muscles and having a fistulotomy carries a high risk of causing incontinence.
This involves cutting or scraping out the fistula and covering the hole where it entered the bowel with a flap of tissue taken from inside the rectum, which is the final part of the bowel.
This has a lower success rate than a fistulotomy, but avoids the need to cut the anal sphincter muscles.
Bioprosthetic plug
Another option in cases where a fistulotomy carries a high risk of incontinence is the insertion of a bioprosthetic plug.
This is a cone-shaped plug made from animal tissue that is used to block the internal opening of the fistula. Some studies have suggested this may be an effective treatment for anal fistulas, but more evidence is needed to be certain.
The National Institute for Health and Care Excellence (NICE) currently recommends carrying out the procedure as part of medical research.
Read NICE guidance on closure of anal fistula using a suturable bioprosthetic plug.
LIFT procedure
The ligation of the intersphincteric fistula tract (LIFT) procedure is a relatively new treatment for anal fistulas.It's designed as a treatment for fistulas that pass through the anal sphincter muscles, where a fistulotomy would be too risky.
During the treatment, a cut (incision) is made in the skin above the fistula and the sphincter muscles are moved apart. The fistula is then sealed at both ends and cut open so it lies flat.
This procedure has had some promising results so far, but it's only been around for a few years, so more research is needed to determine how well it works in the short and long term.
Fibrin glue
Treatment with fibrin glue is currently the only non-surgical option for anal fistulas.
It involves your surgeon injecting a special glue into your fistula while you're under a general anaesthetic. The glue helps seal the fistula and encourages it to heal.
It's generally less effective than fistulotomy for simple fistulas and the results may not be long-lasting, but it may be a useful option for fistulas that pass through the anal sphincter muscles because they don't need to be cut.
Risks of anal fistula surgery
Like any type of treatment, treatment for anal fistulas carries a number of risks.
The main risks are:
The level of risk will depend on things like where your fistula is located and the specific procedure you have. Speak to your surgeon about the potential risks of the procedure they recommend.